
Sometimes, Kristine Yaffe will hear a poignant question from someone at her memory clinic. “I walk five miles a day, don’t drink and play bridge,” they’ll say, “so why do I have Alzheimer’s disease?”
How common is Alzheimer’s? Blood-test study holds surprises
Yaffe, a neurologist and dementia specialist at the University of California, San Francisco, finds it difficult to explain that even if someone does everything they can to lower the risk of dementia, there’s no guarantee they’ll avoid the condition.
Her struggles mirror a challenge in her field. Studies have identified a list of virtuous lifestyle choices associated with a reduced dementia risk, including a healthy diet, physical exercise and social and cognitive stimulation. Research has also pointed to some less obvious factors linked to lower risk, such as treating vision and hearing loss and, potentially, receiving a shingles vaccine. The trouble is that it’s hard to work out how much doing any — or all — of these things helps to reduce risk in the real world.
That’s not for lack of trying. A growing number of ambitious clinical trials have tested the effects of lifestyle interventions, providing people with intensive help to improve their diet, exercise regime, social connections and heart and brain health. These include the FINGER trial1, which involved some 2,650 participants testing a two-year lifestyle overhaul in Finland, and the multimillion-dollar POINTER study2, which tested a similar approach in the United States. These and other studies have suggested that lifestyle programmes can boost cognitive performance.
But these intensive interventions seem to help only slightly — a benefit equivalent to a modest boost on some memory tests. None has been shown to reduce the incidence of dementia, and critics argue that such programmes are costly and difficult to scale up.
Other trials, including offshoots of the FINGER study in the Netherlands and in 12 Latin American countries, will announce their results this month, and the World Health Organization will release its new dementia risk-reduction guidelines on 16 July. Deciphering the most effective ways to cut risks is important for researchers, clinicians and the public alike — especially given that the number of people with dementia worldwide is expected to soar in decades to come.
Blood test holds promise for predicting when Alzheimer’s symptoms will start
Some specialists worry that implementing lifestyle interventions won’t move the needle much; others argue that any reduction in the cognitive decline is worth the effort. Another concern is that researchers are over-emphasizing personal responsibility, when many important contributors to risk — such as air pollution and access to education and healthy food — are mostly outside people’s control. “This is a societal issue,” says Edo Richard, a neurologist at Radboud University Medical Center in Nijmegen, the Netherlands. “I think the focus has been too much on the individual lifestyle.”
Difficult calculations
The number of people with dementia — of which Alzheimer’s disease is the most common form — is expected to grow from 57 million in 2019 to 153 million by 2050, according to the Global Burden of Disease Study3, which collects figures on ill health. More than 60% of people with dementia lived in low- and middle-income countries in 2021 and that is where the burden is growing fastest, partly because of increases in life expectancy.
When it comes to risk factors, probably the most comprehensive synthesis of evidence has come from the Lancet Commission, a group of specialists convened by The Lancet in 2015 to assess research on the condition. “It’s become the Bible, really, to everybody,” says Henry Brodaty, a dementia researcher at the Centre for Healthy Brain Ageing at the University of New South Wales in Sydney, Australia.
The commission’s most recent report4, published in 2024, listed 14 risk factors for dementia that, unlike age or genetics, can be modified. These are a lack of physical activity, high blood pressure (hypertension), obesity, diabetes, smoking, depression, traumatic brain injury, air pollution, less education, social isolation, hearing loss, untreated vision loss, high levels of low-density lipoprotein cholesterol and high alcohol intake (more than about two bottles of wine a week).
By calculating the proportion of dementia cases attributable to each of the 14 risk factors and adding them up, the group estimated that 45% of cases globally could — in theory — be prevented (see ‘Dementia risk factors’).
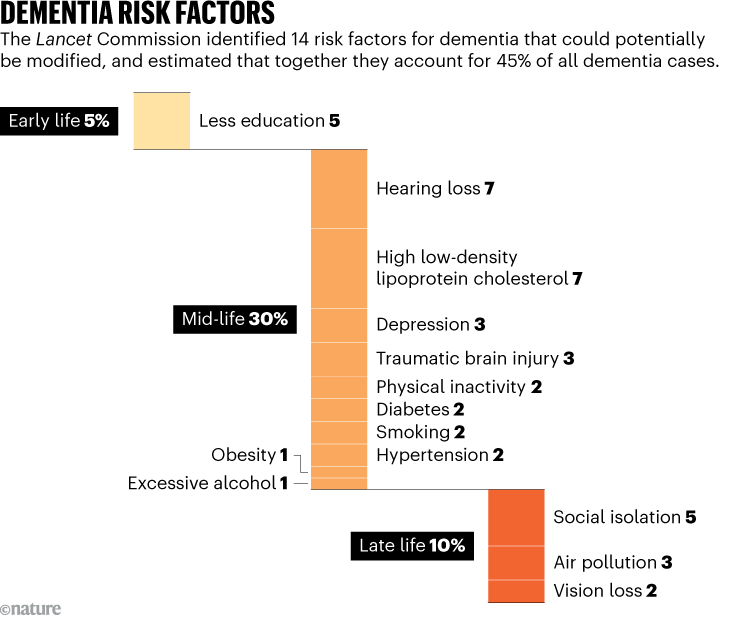
Source: Ref. 4
That bold calculation was based on population-level observations. An individual who tries to eliminate these factors will not reduce their personal risk of dementia by 45%; there is no guarantee that they will reduce it much at all. And exposure to some of these risks — such as physical inactivity or alcohol drinking — could have occurred over decades. It’s unclear whether changing them in mid-life will undo any damage that’s already been done.
Beyond that, evidence shows that people’s health behaviours are hard to shift. “It’s difficult to change people’s lifestyle, particularly if it’s to avert a risk which may be 20 or 30 years away,” says Richard.
Nevertheless, over the past couple of decades, researchers have been trying to see just how much overhauling people’s health habits can help. In 2009, scientists in Finland started the FINGER study1 — a randomized controlled trial to test whether an intensive effort to improve people’s lifestyles could reduce cognitive decline and the risk of dementia. The country already had a history of running pioneering lifestyle-intervention studies that cut risks of cardiovascular disease and diabetes, so they had the necessary expertise.
Led by Miia Kivipelto, a clinical geriatrician at the Karolinska Institute in Stockholm, the FINGER team recruited people aged 60–77 years who had some risk factors for dementia (such as high blood pressure or low education levels) and randomly assigned them to an intervention or control group.
For two years, the intervention group took part in an extensive series of health sessions. Nutritionists helped the participants to improve their diet and physiotherapists guided them through tailored strength and aerobic exercises at the gym. They worked with psychologists and used computer-based training to boost their memory and performance in other mental tasks and they saw medical specialists to track their weight and blood pressure. The participants also received a social boost because some of the sessions were held in groups. People in the control group received standard health advice and some health monitoring.
The researchers tested what the impact of this ‘multidomain lifestyle intervention’ was on participants’ performance in a standard battery of neuropsychological tests of skills such as memory and processing speed. The main outcome was reported as a change in ‘Z score’, which provides a way of expressing the combined test scores in units of standard deviation. A Z-score increase of one would mean that the participants’ average improved by one standard deviation — a big jump.

China is waging war on Alzheimer’s. What can its approach teach the rest of the world?
The findings1, published in 2015, showed that after two years, the intervention group’s average change in Z score was 0.20 and the control group’s was 0.16. That both groups improved “was a big surprise for us”, says study co-author Alina Solomon, a neuroepidemiologist at the University of Eastern Finland in Kuopio. This could be because the participants got better at cognitive tests with practice during the trial.
But that makes interpreting the results more difficult. The intervention group improved by 0.04 more than did the control group (25% better in relative terms), which was statistically significant according to the researchers’ tests. The FINGER team highlights this 25% figure on its website — along with other favourable trial outcomes for the intervention group, such as small improvements in processing speed and a reduced risk of cognitive decline. Kivipelto says that expressing the improvement as a relative percentage change is standard practice in the field. She and her colleagues acknowledge that the effect was small in real terms, but point out that new Alzheimer’s drugs that target amyloid-β protein have also produced only small effects on cognitive function5. “In our field, for brain health and dementia, all the effect sizes are small,” Kivipelto says.
But some researchers use stronger terms to describe the effect of 0.04 on the cognitive tests. “A very small thing,” says Richard. “Tiny,” says Hussein Yassine, who studies nutrition and dementia at the University of Southern California in Los Angeles. One way of thinking about the 0.04 improvement in brain function is that there is a roughly 54% chance that a person picked at random from the intervention group will have a higher score on the cognitive tests than a person picked at random from the control group. It would be 50% if the intervention did nothing.
Fingers extending
A series of other trials have tested similar interventions, with mixed and modest results. In 2017, Kivipelto established the World-Wide FINGERS network, which now includes teams in 73 countries. “In large studies where the intervention is intensive enough, we see consistently these small but significant effects,” says Mariagnese Barbera, scientific coordinator for FINGER at the University of Eastern Finland.
One trial that attracted attention when it was published last year is the POINTER study2, which tested the FINGER approach in the United States. Researchers including Kivipelto randomly assigned around 2,000 people aged 60–79 who had dementia risk factors to one of two groups. One received a ‘structured’ intervention: 38 meetings with specialists over two years in a programme designed to boost exercise and improve diet, cognition and cardiovascular health. The control group received a less intensive, self-guided intervention, which encouraged lifestyle changes but included only six meetings.

The benefits of a healthy diet extend beyond dementia risk, but habits can be hard to change.Credit: Getty
Again, both groups improved on a battery of cognitive tests and the structured intervention group improved marginally more than did the self-guided one. The researchers compared the change in scores in the more intensive intervention group with the expected cognitive decline of people of the same age, and estimated that it slowed down cognitive ageing by one to two years.
But some researchers are unconvinced by the POINTER team’s estimate of slowed cognitive ageing. With such a small difference between test groups, “another interpretation, frankly, is that neither worked”, says Yaffe, who ran a personalized intervention trial involving some 170 people called SMARRT, which also reported a modest effect on cognitive score6.




